From Lewis Blevins MD, Adrenal World News cofounder, medical director of the California Center for Pituitary disorders and professor of neurological surgery at UCSF – I always suggest that a diagnosis of PsuedoCushing’s syndrome be evaluate by a qualified expert who can review findings and either confirm or refute the diagnosis. This applies to even qualified experts in the field. No one is immune to this recommendation. I’ll share a case with you that was misdiagnosed by two endocrinologists. The patient has given permission to share her findings.
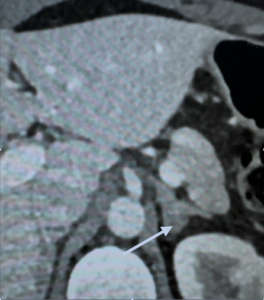
A 47-year-old woman presented with an incidentally-detected 1.4 cm left adrenal adenoma on an MRI done for “preventive purposes.”
She was seen by an endocrinologist who elucidated complaints including insomnia, weight gain of 40 pounds over two years that did not respond to treatment with a GLP-1 drug, and a change in facial appearance.
On physical examination she was noted to be overweight with mid central weight redistribution but had no other specific cushingoid features. Her blood pressure was normal.
Initial diagnostic tests showed:
03/2025
- Plasma renin 3.9 ng/mL/h
- Aldosterone 9 ng/dL
- DHEA-S 178 mcg/dL
- Cortisol 20.3 mcg/dL
- ACTH 57 pg/mL
- 24h UFC 67.5 mcg, Creatinine 1.7g
The above results suggest a diagnosis of ACTH-dependent hypercortisolism. It remains to be determined if this is real Cushing’s or PseudoCushing’s.
Additional studies were performed over the ensuing months.
04/2025 DST
- Cortisol 7.7 mcg/dL
- Dexamethasone 186 ng/dL
- 05/2025
- 24h UFC 73.1 mcg; Creatinine 1.6g
- 07/2025
Salivary cortisol levels on three separate occasions: 0.08, 0.11, 0.07 mcg/dL
07/25 DST
- Cortisol 1.7 mcg/dL
- Dexamethasone 346 ng/dL
- 08/2025 DST
- Cortisol 8.9 mcg/dL
- Dexamethasone 147 ng/dL
- Cortisol 12.7
- Dexamethasone 194 ng/dL
- Cortisol 7.1 mcg/dL
- Dexamethasone 102 ng/dL
I find it unnecessary to do repetitive dexamethasone suppression tests unless dexamethasone levels are not adequate. Did the treating physician expect a different result? In my opinion, thee result confirm pathologic hypercortisolism.
The endocrinologist evaluating the patient diagnosed PseudoCushing’s syndrome.
The patient was then seen at a tertiary medical center for evaluation. It seems as if the prior DST’s were not enough. So, they performed another one. And this one was normal.
09/2025 DST
- Cortisol 1.1 mcg/dL
- Dexamethasone 348 ng/dL
- The physician arranged for a desmopressin stimulation test which can be used to differentiate between neoplastic and non-neoplastic hypercortisolism.
- ACTH rose from 32 pg/mL to 51 pg/mL
- Cortisol rose from 11mcg/dL to 19.3 mcg/dL
Based on standard criteria, it would seem clear that it is far more likely than not that this patient had Cushing’s disease rather than pseudoCushing’s syndrome. Yet the endocrinologist diagnosed pseudoCushing’s syndrome.
The patient sought another opinion and came to see me at UCSF. All the results were reviewed and felt to be highly suspicious for and ACTH-dependent cause of hypercortisolism.
I obtained an MRI that illustrated a right-sided pituitary adenoma.
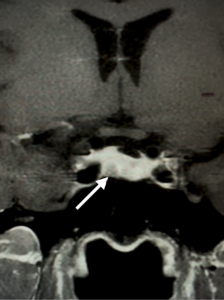
The patient underwent transsphenoidal pituitary surgery at UCSF in late December 2025. Pathology confirmed an ACTH-producing corticotroph adenoma.
In patients who undergo resection of an ACTH-producing tumor we expect postoperative adrenal insufficiency as the remaining normal or nontumoral ACTH-producing cells in the pituitary gland have been suppressed due to the hypercortisolism. The low cortisol levels after surgery are proof of concept and conform that a patient is in remission. The immediate postoperative cortisol level in this patient was undetectable. The cortisol level 6 weeks after surgery was low at 1.9 mcg/dL. She has been treated with steroid replacement. The requirement for steroid replacement varied depending on several factors but averages 11 months.
The patient clearly had ACTH-dependent hypercortisolism due to an ACTH-secreting pituitary adenoma. Her presumed left adrenal nodule and hyperplasia are likely due to chronic stimulation by ACTH secreted by her pituitary tumor.
In this case, the expert second opinion agreed with the endocrinologist in private practice who felt the patient had pseudoCushing’s syndrome. I overruled both of their opinions, and the patient has had successful surgery for an ACTH-secreting pituitary adenoma.
© 2026, AWN. All rights reserved.