
From the desk of Lewis S. Blevins, Jr. MD – A 52-year-old man was referred to the pituitary clinic for further evaluation of hypercortisolism.
Has had an unspecified weight gain and hypertension. His blood pressure was well-controlled on medications. He was slightly overweight but had no typical Cushingoid features.
His 24 h urine free cortisol excretion rate was elevated at 76 mcg. His ACTH level was low measuring 9 pg/mL. His serum cortisol result for the 1mg overnight dexamethasone suppression test was abnormal measuring 1.9 mcg/dL; normal would have been less than 1.8 mcg/dL.
The fact that his ACTH was low indicates the hypercortisolism was ACTH-independent and likely related to an underlying adrenal condition. His DHEA-S level was not checked. It would likely also have been low. The differential diagnosis included functional adrenocortical adenoma, bilateral adrenal hyperplasia, and adrenocortical carcinoma.

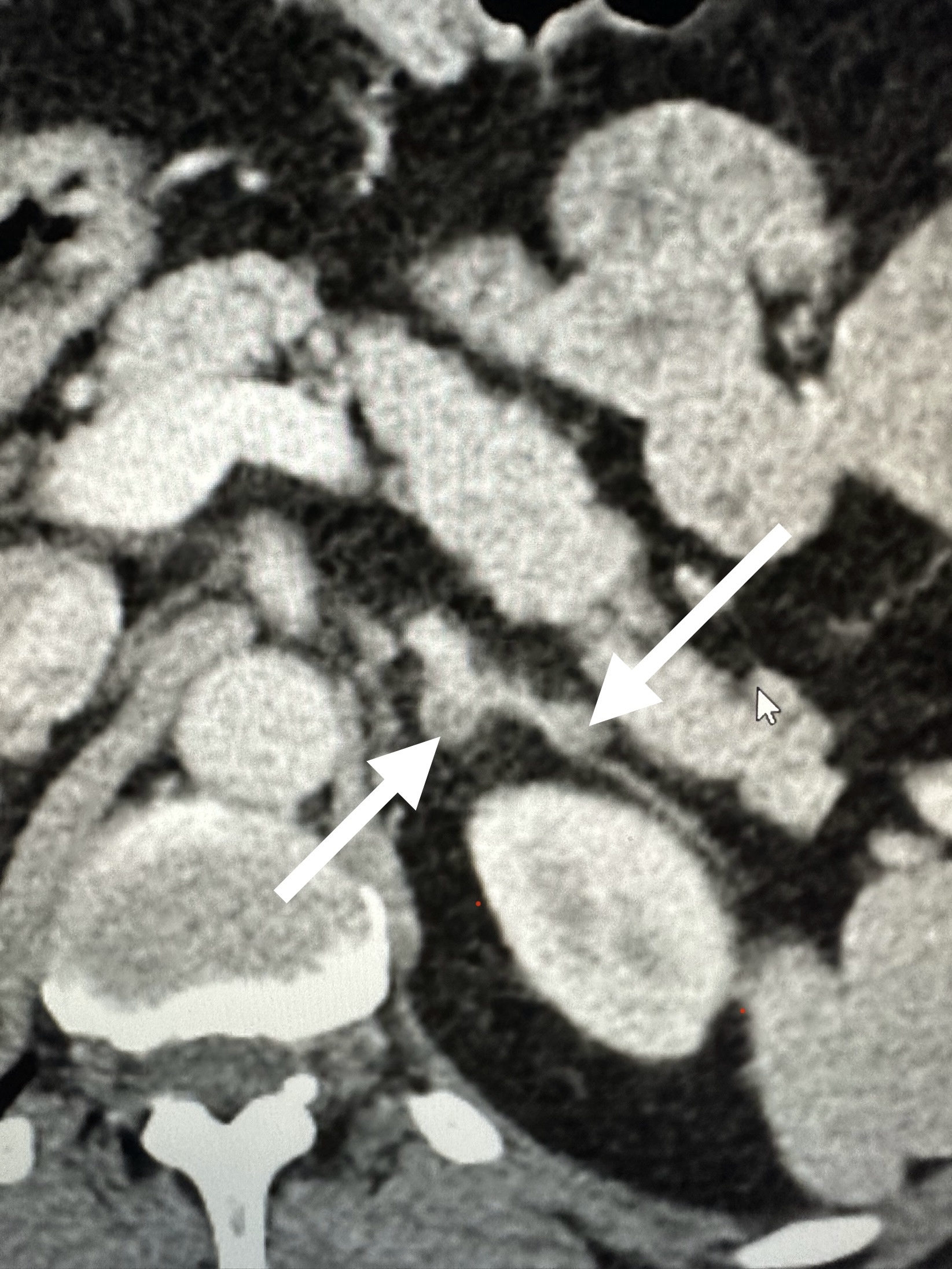
CT of the adrenal glands demonstrated bilateral adrenal nodules. The largest nodule measured 1.9 cm.
Cortisol excretion in adrenal hyperplasia may range from barely detectable, a condition often called mild autonomous cortisol secretion (MACS), to moderate or even marked. Degree of cortisol overproduction and duration of disease, coupled with other risk factors for conditions like metabolic syndrome and hypertension, influence the overall clinical picture.
Adrenal nodular hyperplasia may be due to a number of different conditions. Nodular adrenal hyperplasia is characterized as micronodular, macronodular, or massive macronodular. PPNAD, discussed elsewhere, is usually associated with small nodules and is often due to a mutation in the PRKAR1A gene. Other germline and sporadic somatic mutations have been described in the ARMC5, GNAS, and PDE8B genes. The ARMC5 gene seems to be the most common of these mutations. It appears to be a tumor suppressor gene.
Left untreated, patients are at risk for a number of complications including deep vein thrombosis, coronary artery disease, stroke, peripheral vascular disease, diabetes mellitus, hypertension, infections, osteoporosis, and depression.
Treatments for hypercortisolism due to bilateral adrenal hyperplasia include medications and surgery. Medications that block cortisol synthesis are often effective. Surgery can involve removal of the largest adrenal gland, both glands, or removal of some of the largest nodules. I do not usually recommend the procedures that remove the largest nodules only. My patient elected a trial of therapy with one of the commonly employed inhibitors of cortisol production.
© 2026, AWN. All rights reserved.